Did You Know?


This is where ASA classification can help. An ASA risk is a 1-to-5 score adapted for animals from human medicine’s American Society of Anesthesiologists. The system is based on the patient’s overall health, not the procedure being performed.
The ASA scoring system is NOT an assessment of total perianesthetic or perioperative risk, since many things, including the surgical procedure planned, the skill & training of the anesthetist and the surgeon, as well as the the resources at hand, contribute to the entirety of operative risk. If you EVER have any questions or concerns regarding your pet and any upcoming procedure they may be having talk to your veterinarian/veterinary support staff immediately!
The pre-anesthestic phase includes NOT only the choice of preanesthetic sedatives & analgesics but also a full preanesthetic evaluation & stabilization of the patient, if necessary. Categorization of patients using the American Society of Anesthesiologists (ASA) provides a framework for evaluation of patient health & determination of stabilization requirements prior to anesthesia.
| STATUS | ASA CLASSIFICATION | EXAMPLES |
| I | Healthy Pet, No Disease | Elective Spay/Neuter |
| II | Mild systemic disease or localized disease | Healthy geriatric pet, mild anemia or obesity |
| III (Fair) | Moderate systemic disease limiting activity but NOT life-threatening | Mitral valve insufficiency, collapsing trachea, poorly controlled diabetes |
| IV (Poor) | Severe systemic disease, incapacitating; life-threatening; not expected to live without surgery | Hemoabdomen from splenic rupture, severe traumatic pneumothorax, organ failure |
| V (Grave) | Moribound; not expected to live >24 hours, with or without surgery | Multi-organ failure, severe shock, terminal malignancy |

DISCLAIMER: These are COMMON medications/adverse reactions to veterinary anesthetic medications, just like humans, pets also can have a variety of symptoms/reactions that are not listed or documented.
If you have any questions or concerns always speak to your veterinarian about the kinds of medications utilized and the potential side effects that may occur.
| Anesthetic/Analgesic Drug | Common Adverse Effects |
| Dexmedetomidine Medetomidine Xylazine | BradycardiaCardiac Output ReductionHypertension/HypotensionVasoconstriction |
| NSAIDs Steroids | Bleeding DisorderDiarrhea/VomitingGastrointestinal UlcerationLethargyRenal/Liver Failure |
| Diazepam Midazolam | Minimal Cardiorespiratory EffectsParadoxical Excitement of Patients |
| Halothane Isofurane Sevofurane | Decreased Cardiac OutputDecreased Myocardial Contractility Hypothermia/HyperthermiaMay result in hypotensionVasodilation |
| Diazepam/Ketamine Propofol Tiletamine/Zolazepam | CyanosisOccasional Muscle Twitches/SeizuresProfuse Salivation/Airway SecretionsRespiratory Depression Transient TachycardiaVasodilation |
| Bupivacaine Lidocaine Mepivacaine | BradycardiaHyperthermia in some animals; hypothermia more likelyCardiac ArrestHypotensionSeizure |
| Buprenorphine Butorphanol Fentanyl Hydromorphone Morphine | BradycardiaMydriasis/MiosisRespiratory Depression (hypoventilation, apnea)Vomiting |
Cary Craig
Health Science Associate Clinical Professor
Surgical & Radiological Sciences UC Davis Veterinary School
There are no medical contraindications to any anesthetic technique in CH. However, I think there are considerations, particularly with respect to recovery from general anesthesia. My preference would be to use short acting or reversible techniques. Inhalant anesthetics such as isoflurane have the advantage of being very short acting and recovery is rapid once the inhalant is discontinued. My own CH kitties I have induced anesthesia either with propofol (a short acting injectable anesthetic) or isoflurane or sevoflurane by mask. For anesthetic maintenance gas anesthesia is best, maintaining anesthesia with injectable anesthetics for a spay would require doses that would prolong the recovery period. The gas should be delivered by an endotracheal tube rather than a facemask. Anesthetized animals, with or without CH, cannot protect their airways and are at risk for aspiration and/or airway obstruction. I would also recommend the use of an analgesic (pain control medication) and it is best used as a premedication, i.e., given prior to the surgical procedure. Usually this is a narcotic. The doses used for pain control are safe. Occasionally, some cats have some behavioral changes when they are given narcotics which can be sedation, euphoria or dysphoria. These are temporary; they go away as the drug wears off. If the drug effects are unacceptable the narcotic can be reversed.
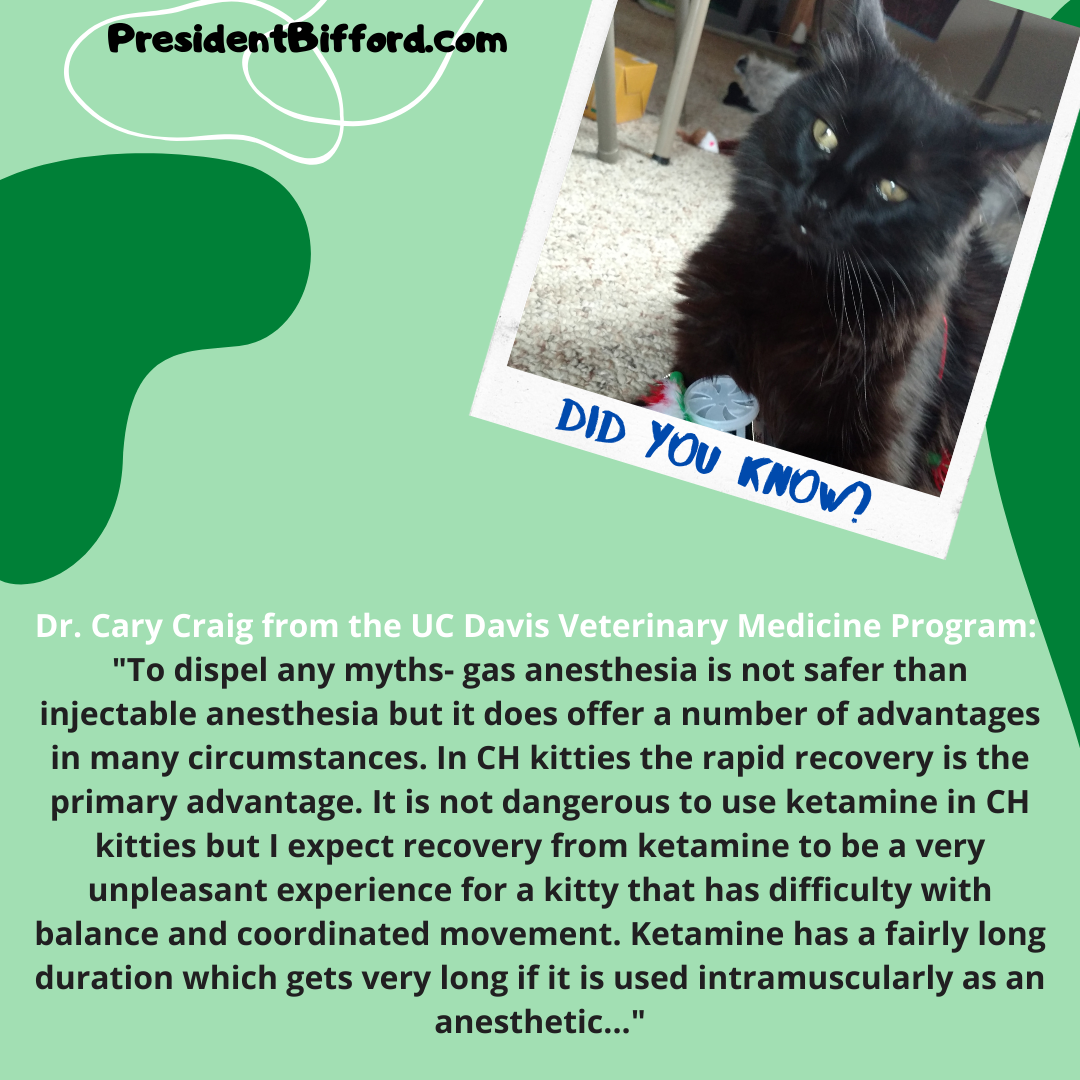
To dispel any myths- gas anesthesia is not safer than injectable anesthesia but it does offer a number of advantages in many circumstances. In CH kitties the rapid recovery is the primary advantage. It is not dangerous to use ketamine in CH kitties but I expect recovery from ketamine to be a very unpleasant experience for a kitty that has difficulty with balance and coordinated movement. Ketamine has a fairly long duration which gets very long if it is used intramuscularly as an anesthetic.
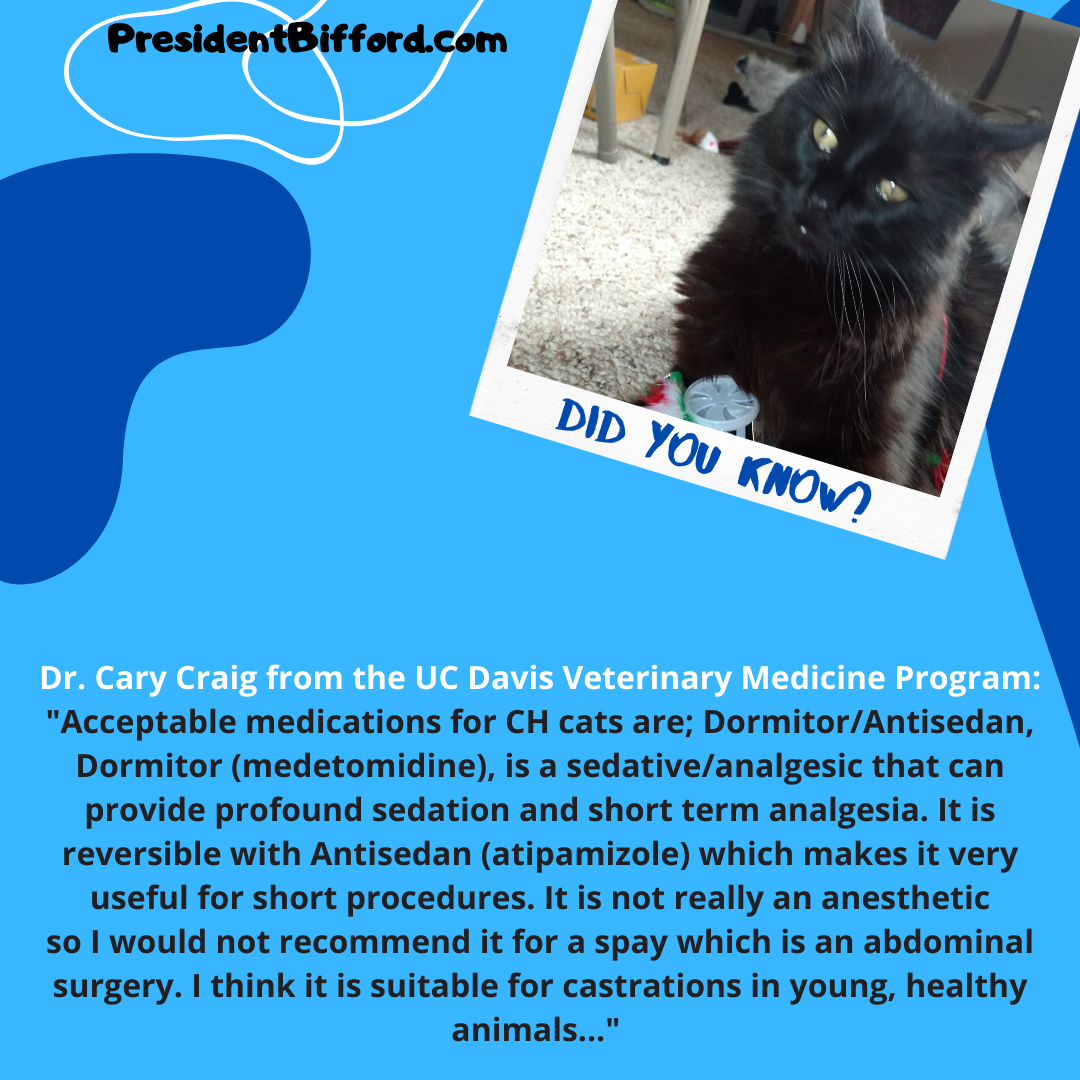
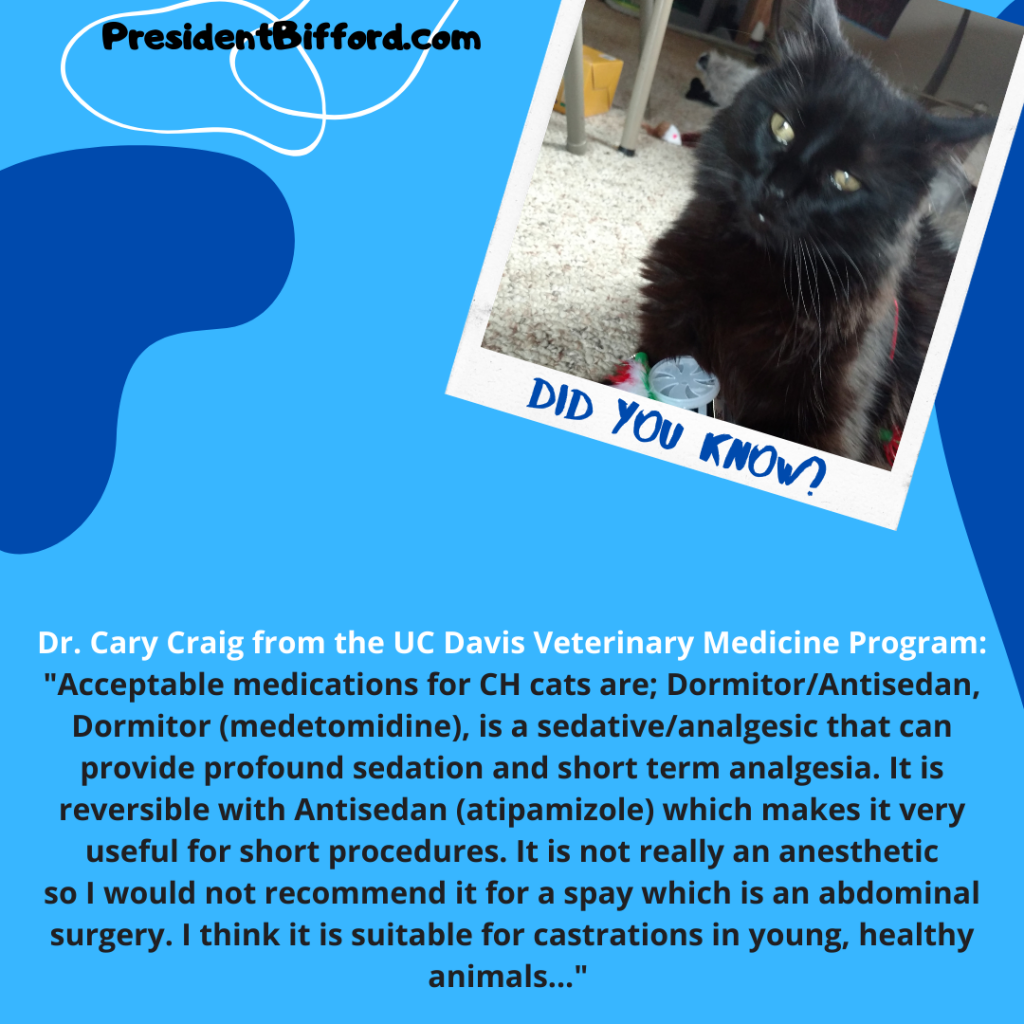
Acceptable medications for CH cats are; Dormitor/Antisedan, Dormitor (medetomidine), is a sedative/analgesic that can provide profound sedation and short term analgesia. It is reversible with Antisedan (atipamizole) which makes it very useful for short procedures. It is not really an anesthetic so I would not recommend it for a spay which is an abdominal surgery. I think it is suitable for castrations in young, healthy animals.
Neurologic injury from anesthesia is caused by a period of inadequate oxygen delivery to the brain. The severity of the neurologic damage is proportional to the length of time the brain is oxygen deprived. The part of the brain involved in vision is particularly sensitive to lack of oxygen so blindness is the most common symptom, more severe deficits are certainly possible.
There are basically two reasons why the brain would not get enough oxygen during anesthesia in all patients (normal or otherwise) and with all anesthetics (there are no safe anesthetics, only safe anesthetists):
I think one of the most common causes for a cat to wake up with neurologic problems is a prolonged period of very low blood pressure. If not enough oxygen gets to the lungs so that there is not enough in the blood the gums and pink skin will turn bluish purple (cyanotic) and if anyone is looking at the cat they should see this. If there is enough oxygen in the blood but not enough is getting to the brain you have no way of knowing this unless you are measuring blood pressure. It can even happen sometimes when blood pressure seems ok – blood flow is extremely important and we infer blood flow from blood pressure. So it is important that the person monitoring the anesthesia can interpret the blood pressure numbers in the context of the cat’s clinical signs of adequate blood flow.
There are still too many practices that do not routinely measure blood pressure in their anesthetized patients with the assumption that standard drug protocols and dosages won’t cause a problem. But normal doses in normal patients can, and often do, cause problems. If the problems are detected and addressed they are not serious. If not detected there may have serious consequences.
This is scary stuff but it should not stop client’s from having their cat’s anesthetized for necessary procedures (e.g. spay, neuter). The incidence of cats that aren’t ill dying while anesthetized has been found to be about 0.3% (or 175 out 80,000). That figure goes up substantially if the cat is sick when it is anesthetized. This is much better than 10 or 15 years ago (but still ten times the mortality rate seen in people) and we are working very hard at finding ways to make it even better.
I think the most important factors in improving the safety of anesthesia are experience with the drugs being used and in anesthetizing the species they are being used in, experience and skill with endotracheal intubation and vigilant monitoring.

Dr. Phil Zeltzman, brought to you by IDEXX & Pet Health Network
There are many urban legends surrounding surgery and cats. Here I take a rational look at 8 stubborn myths I encounter regularly.
1. Myth: “My cat is too old for anesthesia”
You should think twice when your friend or the internet tells you that your cat is too old or sick for anesthesia, and don’t be afraid to seek out an expert about this concern. If your cat is that old, surgery is probably not being recommended just for fun. Your veterinarian is probably talking about performing surgery because of a serious reason or even a life or death situation.
A complete physical exam and blood work should always be performed before anesthesia. In older cats, it may be wise to also take chest and belly radiographs, as well as an ECG to be thorough. Some patients may need to be stabilized before anesthesia, which may mean correcting blood work imbalances, giving IV fluids or giving a blood transfusion prior to anesthesia and surgery.
2. Myth: “Surgery is painful”
This is actually a true statement. However, surgical pain should not be ignored in 2015. We have many safe pain medications to choose from to treat pain before, during and after surgery. We should also remember that depending on what your cat’s condition is, she is most likely already in pain, which will continue to stay the same or worsen without surgery. The goal of surgery is often to decrease pain.
3. Myth: “There is no point if there is no cure”
This mostly relates to cats with a tumor. It is a matter of opinion and expectations. And it’s a very personal decision.
Without the benefit of a biopsy, we don’t know whether a mass is cancerous or benign until it is removed and analyzed. Even when a mass is cancerous, it doesn’t necessarily mean that it’s the end of the road.
Ultimately, your decision should not be based only on quantity of life (or survival), but mostly on quality of life.
Ironically, sometimes, the situation doesn’t depend on whether a mass is benign or cancerous, but on where it is located. A perfectly benign mass blocking the windpipe, the esophagus (the tube between the mouth and the stomach) or the urethra (the tube between the bladder and the outside world) will have life-threatening consequences.
4. Myth: “My cat will not survive confinement”
Confinement is often required after surgery. The time required depends on the procedure. Confinement may be in a crate, an upside down baby/puppy play pen, a “cat tent,” a small room or part of a room. It may seem cruel to some, yet preventing jumping and running is critical to allow proper healing. Cats don’t know what is best for them. You should.
Interestingly, most cat guardians I deal with regularly tell me that in the end, confinement was easier than they expected.
5. Myth: “I can’t keep a plastic cone on my cat”
Sure, a plastic cone can be a royal pain depending on how stubborn your cat is. But this “necessary evil,” worn for two weeks, is not nearly as bad as another surgery to stitch up a chewed incision. And it sure is cheaper than paying for this second surgery!
There are a few alternatives to the standard “lamp shade” or Elizabethan collar such as neck braces or inflatable “donuts.” Not all of these options will work, depending on where the incision is located, so alternative options must be discussed with your surgeon or family veterinarian.
6. Myth: “There’s always a cheaper way”
Sure, you can get to work in a beat-up truck or in a Ferrari. You can go to work in worn-up, second-hand clothes or in a tailor-made suit. But when it comes to surgery, the choices are suddenly much more important. Seeking the cheaper surgery may not be in your cat’s best interest. Which corner do you want to cut? Not give pain medications? Not give antibiotics? Not use sterile equipment? Unfortunately, good equipment, good staff and good skills cost money. And this is reflected in the cost of surgery. The good news is you can get an insurance plan for your dog to avoid this financial dilemma.
7. Myth: “I can just use medication instead”
I am very sorry to say that I have met cats with megacolon (a painful condition due to many months of severe constipation) and other long-term conditions that had been treated “medically” (i.e. with medications) for months to years. These cats suffer on medications, while surgery could have provided much better results. Initially, the medications only address the signs, until they don’t. Surgery addresses the cause of the condition.
As I always say, “the disease is the enemy. Surgery is your friend.”
8. Myth: “Things will get better on their own”
The difficulty is that you cannot tell if vomiting is a sign of something benign or something serious. Sometimes, vomiting is due to eating a bit too much or a bit too fast. And sometimes, vomiting is due to a foreign body which requires surgery to be removed. So don’t procrastinate; seek help from your family vet sooner rather than later. Waiting too long can have devastating consequences on your cat’s health.
These 8 myths are not meant to offend anyone. They are based on observations made over years of practice. Sure, there are complications, expected or not, during and after surgery. Fortunately, most of the time, surgery can make a world of difference for your cat.
Questions to ask your veterinarian about surgery:
If you have any questions or concerns, you should always visit or call your veterinarian — they are your best resource to ensure the health and well-being of your pets.